ORIGINAL ARTICLE
The Fire is Coming: An HIV Prevention Intervention Contextualized to the Maasai People of Tanzania
Holly Freitasaand Marcia A Nayakb
Abstract
“The Fire is Coming” film is an innovative HIV-prevention intervention contextualized to the Maasai people of Tanzania through use of a traditional Maasai story. The intervention was developed and implemented in partnership with Maasai Pastoralists for Education and Development (MAPED). Although there have been numerous Knowledge-Attitude-Practice (KAP) surveys conducted among the Maasai, this is the first control-group comparison study designed to measure the effectiveness of an HIV-prevention intervention contextualized specifically to the Maasai people of Tanzania. We will first discuss the background and context in which the intervention was developed and methods used to develop the intervention. We will then discuss the evaluation methods, results, and implications of a retrospective Knowledge, Attitudes, Practices (KAP) two-village comparison survey (n=200) for “The Fire is Coming” HIV-prevention intervention among Maasai people. There was a significant effect for HIV-related attitudes, t(16) = 2.77, p <0.05, regarding willingness to care for an HIV infected person, willingness to be tested for HIV, self-efficacy toward HIV-prevention, married women’s ability to use condoms, unmarried girls’ ability to refuse high-risk sexual behaviors, married men’s ability to use condoms, and married men’s ability to limit sex to their spouses. There was a significant effect for HIV-related behavior changes, t(8) = 2.89, p <0.05, with reported family decisions made, esoto (the ritualized sexual initiation of pre-pubescent girls) stopped, sexual behaviors changed, blade-sharing stopped, and other traditional custom changes reported. Although knowledge rates were often higher in the intervention area than in the comparison area, there was no significant difference in HIV-related knowledge, t(12)=1.85, p >0.05. Implications: Belief in one’s ability to do something is often the pivotal point for behavior change. The results of the survey denote a highly effective intervention in changing HIV-related attitudes and behaviors. It is promising for replication among other Maasai communities and for adaptation with indigenous people groups in other regions.
Background and Context
HIV infection rates are rapidly rising in Maasai regions.1,2 Although actual HIV rates are difficult to obtain due to governmental restrictions on census and data collection differentiation by tribal identification, sexual traditions and social norms place the Maasai people of Tanzania at high risk for sexually transmitted diseases. Maasai norms and traditions include esoto (coerced sexual initiation of pre-pubescent girls), encouragement of multiple sexual partners among teenage males, polygamy, marriage of young girls to older men, wife sharing, the obligation for wives to show hospitality by engaging in sexual behaviors with traveling male visitors, and male circumcision using a common blade.1,2,3,4 Among the Maasai, the exchange of reproductive fluids is considered essential to both mental and physical health; intentionally high levels of procreation limit the acceptability of condom use for either birth control or prevention of sexually transmitted disease.1,2
Significant barriers to health education messages have resulted in limited HIV-related knowledge, misconceptions regarding HIV, and continuance of high-risk, HIV-related behaviors. Language, limited education, and distance from health services make up some of the barriers that keep Tanzania’s national efforts to reduce HIV transmission from reaching the Maasai people. Approximately 20% of Maasai people speak the national language or have any formal education.5 All public health campaigns in Tanzania, including HIV education, are conducted in Swahili, leaving non-Swahili speakers uninformed.4,6 Furthermore, all national HIV surveillance efforts, including KAP studies, have been conducted in Swahili,7 leaving non-Swahili speakers uncounted, their voices unheard, and their plight unknown to both national and international organizations concerned with HIV and AIDS.8,9 Most Maasai people in Tanzania live in rural areas distant from city hubs where HIV prevention, testing, and treatment services can be obtained. Poorly conditioned and infrequently traveled roads limit public transportation. Maasai people generally travel by foot or in the open-bed of delivery trucks on weekly transportation routes from the village areas to the city hub and back.
Additional barriers limit the effectiveness of standard ABC (abstinence, be faithful, and condom) messages.2,4,10 Many Maasai people believe that they, as a people group, are immune to HIV or that their traditional medicines will cure the disease. The lack of accessibility and acceptability of condoms further complicates the effectiveness of the ABC message.4,11 Finally, many of the commonly used HIV education methods, which promote individual behavioral change are rendered ineffective within the traditional Maasai top-down and group-level decision making structure.2,4,6
In late 2006, a small Maasai organization, MAPED (Maasai Pastoralists for Education and Development), of the Olbili sub-village in Simanjioro District, Tanzania, became aware of the threat of HIV. Intent on protecting their people, they sought HIV education. In 2007, sixteen of their young Maasai warriors attended an intensive HIV training course which met both international and Tanzanian HIV education standards. The young warriors recognized the dangers of high-risk Maasai traditions and sexual practices and determined to make changes, not only to protect themselves and their families but also to educate other Maasai about HIV to preserve their tribe.
Intervention and Methods
The young warriors, together with MAPED, determined that a public health education intervention was necessary to inform and educate the Maasai people. In response, an educational program was designed to meet three goals: 1) to bring contextualized HIV prevention education to the Maasai, 2) to increase the awareness of vulnerability to HIV infection due to traditional and common HIV-related behaviors, and 3) to facilitate dialog within Maasai communities that would ultimately result in modification, adaptation, or discontinuation of high-risk, HIV-related behaviors.
A participatory process was used to identify the preferred learning medium for HIV prevention education among the Maasai. It was noted that the existing local public-health education was ineffective in Maasai areas for several reasons. First, written health information is inaccessible to a majority of Maasai who are oral learners. Second, health information given via radio is also inaccessible to a majority of Maasai, because all official public-health announcements in Tanzania are made in Swahili — not the Maasai language. Third, Maasai perceive national public-health announcements in Swahili as non-applicable to themselves because of cultural differences. Through discussions and the review of previous HIV-related KAP studies, the Maasai leaders and HIV education team determined that the preferred learning medium for HIV prevention education was audiovisual and chose to create an educational film using Maasai spokespersons, traditions, and storytelling. A private donor provided a sum of money to Medical Ambassadors International for HIV education in Africa. This donation, in turn, was directed toward the proposed intervention.
The next step in the process was to identify traditional Maasai stories that could effectively convey the HIV-prevention message. Maasai stories were collected from every available source. After review of many stories, a widely-known traditional Maasai story was selected which tells about a foolish man who knew that a great fire was coming across the land, posing great risk to his homestead, family, and animals. After many warnings, the man still did nothing to protect himself and was overwhelmed by the fire. The story elicits much laughter among the Maasai people, and they find re-telling of the man’s obvious foolishness a source of great humor. The story provided a perfectly contextualized analogy to emphasize the importance of HIV awareness and preventive action among the Maasai.
“The Fire Is Coming” video production began in 2008. Maasai elders, political leaders, warriors, and other tribe members were briefed in the basic story-line and then participated to create the unscripted footage, telling the story in their own words, providing HIV prevention education, advocating for change of high-risk cultural practices, and warning of the dangers of ignoring the issue. Film editing was conducted in cooperation between Media 7, a volunteer HIV educator from Medical Ambassadors International, and MAPED. Field-testing was conducted in 2009, and the film was released for facilitated public viewing in the Maasai community in 2010.
The target level of the intervention was the sub-village level, where general decision-making is done and social and behavioral norms are established. A participatory, adult-learning approach was chosen in conducting the intervention. The approach relied on the intervention’s problem-posing nature and on discussions guided by trained volunteer Maasai facilitators from MAPED following public viewings of “The Fire Is Coming” video to achieve the intervention goals of changing HIV knowledge, attitudes, and behaviors in each village.
Evaluation
In 2011, after one year of active implementation by MAPED in the local Maasai community, an evaluation was scheduled as part of the assessment and quality improvement for the on-going program. The aim of the evaluation was to determine the effectiveness of the intervention in bringing contextualized HIV prevention education and awareness to the Maasai people and to influence change in both attitudes and high-risk behaviors associated with HIV transmission. An additional aim of the evaluation was to determine whether the intervention influenced change in cultural and social norms in the intervention area. A baseline study had not been done prior to the beginning of the intervention; therefore, a two-village comparison survey was designed to obtain HIV-related knowledge, attitudes, and behaviors among villagers whose community received the intervention and compare them to survey responses from villagers whose community did not receive the intervention. The evaluative nature of an on-going public health education intervention by a Tanzanian registered non-government organization did not require approval by Tanzania’s Institutional Review Board.
A Knowledge, Attitudes, Practices (KAP) survey instrument was developed for the evaluation using the following operational definitions as defined by Tanzania Commission for AIDS (TACAIDS).
HIV-related knowledge: TACAIDS defines HIV-related knowledge as knowing that: using condoms and having just one uninfected, faithful partner can reduce the chance of getting HIV; a healthy looking person can have HIV; an infected mother can transmit HIV during childbirth and breastfeeding. Additional HIV-related knowledge included rejecting the two most common myths about HIV transmission: “People get HIV from mosquito bites” and “People can be infected with HIV by sharing food with someone sick with AIDS.”7,12
HIV-related attitudes: We adapted questions from the Tanzania HIV/AIDS Indicator survey to measure three areas of attitude regarding HIV/AIDS. 1) accepting attitudes toward those living with HIV/AIDS, 2) attitudes toward negotiating safer-sexual relationships with husband/wife, and 3) attitudes of adults toward educating youth about condoms to prevent HIV.7 Within our definition we also include attitudes toward self-efficacy in reducing HIV risk, vulnerability, or risk in contracting HIV and willingness to be tested for HIV infection.
HIV-related behaviors: The concept of HIV risk behaviors includes all HIV-related behaviors that allow for HIV transmission. These practices include esoto (the ritualized sexual initiation of unwed girls), multiple and concurrent sexual partners of the same or opposite sex, the sharing of blades or sharp instruments that penetrate the skin, and other traditional customs such as sexual hospitality practices.12
The survey included both closed-ended, socio-demographic questions and open-ended questions modified from international and national KAP studies to capture data relevant to Maasai specific HIV-related knowledge, attitudes, and behaviors. Survey questions also assessed HIV-related knowledge (i.e. condom use) that was not directly addressed in “The Fire Is Coming” video intervention, allowing the evaluators to further ascertain the impact of the intervention. Presumably, there would be little if any difference between the intervention and comparison villages on these items. In order to protect informants, no questions regarding personal sexual activity or sexual practices were included in the survey. Survey questions were originally written in English, translated to KiMaasai, and back-translated to ensure understandability and conceptual translation accuracy. Pilot testing and revision of surveys was done prior to data collection to ensure inter-rater reliability and enhance consistency among data collectors. Survey data was collected using semi-structured face-to-face individual interviews conducted in the Maasai language by a trained, bilingual Maasai data collector. Prior to any data collection, MAPED sought and received permission to conduct the survey from village elders and leaders and sub-village leaders. Data collectors received permission from both boma (home cluster) leaders and individuals prior to each interview. Each interview took approximately one hour and occurred over a ten-day period from May 2 to 12, 2011. Intervention and comparison village data were collected simultaneously by four Maasai speaking, trained research assistants, none of whom had visited the villages prior to data-collection.
Sample
A cluster sampling process was used for the evaluation. Two Maasai villages were selected using purposive sampling to control for location, village size, proximity to the city, and available health services. A distance of approximately 200km between otherwise homogeneous villages controlled for potential intervention crossover effect. Within the villages, a convenience sample of 100 respondents each from sub-villages within the intervention and comparison area, respectively (n=200), were surveyed. (Note: All figures represent the number of respondents who directly answered the respective survey questions.) Demographically, there were 54 female and 45 male respondents documented in the intervention area compared with 52 females and 46 males in the comparison area. The age range of study respondents was 13-70 years-of-age, with an average age of 31 years in intervention area and 37 years in the control area. Adolescents were included in the study based on documented cultural norms of very early sexual debut, especially for girls.1 In the intervention area, 73 respondents (11 comparison) reported attendance at an HIV prevention event in their community. Christian religion was claimed by 98 respondents in the intervention area and by 80 respondents in the comparison area.
Results
HIV-related Knowledge
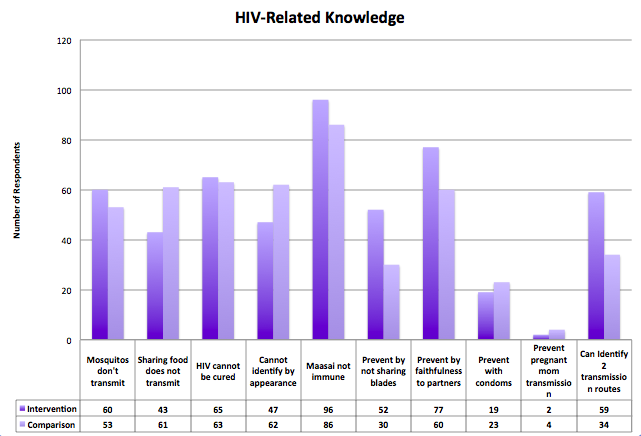
Sixty respondents from the intervention area (34 comparison) were able to correctly identify two routes of HIV transmission, with sexual intercourse and sharing of blades being listed most frequently. In the intervention area, 48 respondents (63 comparison) correctly stated that HIV infection cannot be identified by a person’s appearance (Figure 1).
Two respondents in the intervention area (23 comparison) were unable to identify any HIV transmission routes. Knowledge regarding HIV prevention practices was as follows: abstinence and/or faithfulness to marital partners (77 intervention, 60 comparison), not sharing blades (52 intervention, 30 comparison), and condom use (19 intervention, 23 comparison). In the intervention area, 74 respondents (38 comparison) reported that women are tested for HIV during pregnancy; 34 respondents (21 comparison) said that HIV transmission from mother to infant can be prevented. Two respondents in the intervention area (4 comparison) listed medication as a possible HIV-prevention strategy for mother to child HIV transmission, and 82 respondents (56 comparison) stated that traditional Maasai medicine does not cure HIV. Knowledge that Maasai are not immune to HIV was high in both intervention (96) and comparison village areas (85). A two-tailed t-test was conducted to compare HIV-related knowledge between the intervention and comparison area respondents regarding condom use, faithfulness to partner, HIV-transmission routes, perceived Maasai immunity to HIV, cure by traditional Maasai medicines, and maternal-child transmission. Although on most survey items knowledge rates were higher in the intervention area, there was no significant HIV-related knowledge difference between intervention and comparison village areas, t(12)=1.85, p >0.05.
HIV-related Attitudes
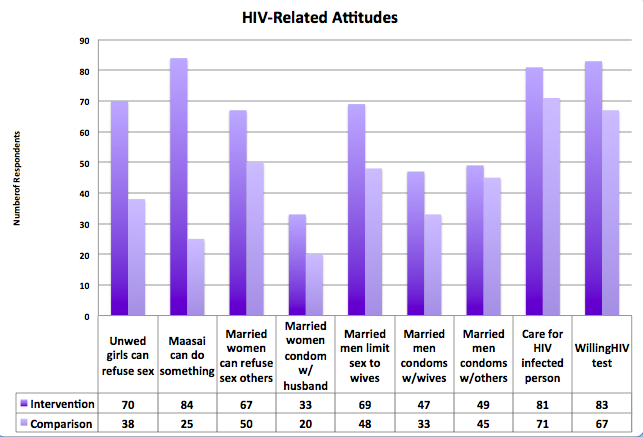
In the intervention area (figure 2), 81 respondents (71 comparison) stated they would care for an HIV infected person. Willingness to be tested for HIV infection was indicated by 83 intervention area respondents (67 comparison); 84 intervention area respondents (25 comparison) stated that Maasai can do something to reduce the risk of HIV. Conversely, 54 respondents in the comparison area stated the belief that Maasai are unable to reduce the risk of HIV. Levels of concern about HIV in the community were “very concerned” (39 intervention; 81 comparison), “concerned” (52 intervention; 8 comparison), and “unconcerned” (8 comparison).
Few respondents agreed that women can refuse sex with their husbands (10 intervention, 10 comparison); however, 67 respondents in the intervention area (50 comparison) stated that women are able to refuse sex with others and can negotiate use of a condom with their husbands (33 intervention; 20 comparison) and with others (53 intervention; 34 comparison). In the intervention area, 69 respondents (48 comparison) reported that married men are able to limit their sexual activity exclusively to their wives.
In the intervention area, 70 respondents (38 comparison) stated that unwed girls can refuse to have sex or participate in esoto. In the intervention area, 37 respondents (39 comparison) stated that unwed girls can buy and use condoms. A two-tailed t-test analysis was conducted to compare the intervention and comparison area respondents’ HIV-related attitudes regarding willingness to care for an HIV infected person, willingness to be tested for HIV infection, self-efficacy toward HIV-prevention, married women’s ability to use condoms, unmarried girls’ ability to refuse high-risk sexual behaviors, married men’s ability to use condoms, and married men’s ability to limit sex to their spouses. There was a significant effect for HIV-related attitudes t(10) = 2.89, p <0.05.
HIV-related Behaviors
Esoto, the ritualized sexual initiation of unwed girls, was reported stopped by 85 respondents (figure 3) in the intervention area (41 comparison). A family decision to decrease the risk of HIV was reported by 59 intervention area respondents (12 comparison). Participants reported they stopped sharing blades (30 intervention; 9 comparison), changed sexual behaviors (60 intervention; 26 comparison), and changed high-risk traditional customs (87 intervention; 47 comparison). A two-tailed t-test analysis was conducted to compare the intervention and comparison area respondents reported behaviors regarding family decisions made, esoto stopped, sexual behaviors changed, blade-sharing stopped, and other traditional custom changes. There was a significant effect for HIV-related behavior changes, t(8) = 2.89, p < 0.05.

Discussion
The most significant attitude difference between the intervention and comparison villages was that of collective self-efficacy, or the belief that they as Maasai people are able to reduce the risk of HIV in their community. Self-efficacy has been found by researchers to be one of the key factors involved in behavior change. Those who believe that nothing can be done are likely to do nothing, while those who believe they are able to do something are significantly more likely to take preventive action. Self-efficacy, or collective self-efficacy in this case, when combined with risk perception translates into behavior change in ways that knowledge alone does not.13 Maddux14 reported data consistent with our findings, that low self-efficacy has been associated with higher levels of anxiety. The high number of comparison area respondents who reported being “very concerned” about HIV is matched with a low number of comparison area respondents who believed that something could be done about HIV. In the comparison area, respondents may have had a perceived helplessness regarding HIV and, therefore, reported the highest levels of concern. Conversely, respondents in the intervention area demonstrated high levels of self-efficacy regarding their ability to reduce the risk of HIV and positive action taken by their community; thus, they reported being “concerned,” but not “very concerned.”
In our attempts to collect and analyze the data, we have applied national standards of comprehensive HIV knowledge, attitudes, and behaviors. However, we must consider the cultural context in which the intervention took place and the very nature of participatory community based research and development.
The hallmark of community-based participatory interventions is a process wherein awareness of an issue is raised in the community; the community then discusses the issue and arrives at culturally appropriate and, therefore, contextualized solutions to the problem. Among the Maasai communities in this study, a great number of families live in polygynous relationships; early and extramarital sexuality has been sanctioned by the society; and a high birth rate is desirable. Solutions that have come from within the Maasai community focus on the reduction and elimination of extramarital sexual partnerships, elimination of blade sharing practices, and mutual encouragement for HIV testing.
In response to the evaluation results, MAPED continues to work toward their goals of HIV prevention with a focus on increasing HIV-related knowledge and strengthening the positive outcomes in HIV-related attitudes and behaviors among Maasai communities. It is within the context of these community developed solutions that Maasai can be successful in changing both attitudes and behaviors that lead to the reduced risk of HIV in the community.
Study Limitations
Although the results of the program evaluation are indicative of a highly effective intervention, we recognize there are limitations to this evaluation study. Selection of a pre-experimental design does not allow us to unequivocally establish a causal relationship between the independent (HIV intervention) and the dependent (HIV-related knowledge, attitude, and practices) variables.15 After controlling for demographics, access to health facilities, distance (to limit cross-contamination), and other variables, we show that there are notable, statistically significant differences between the intervention and comparison Maasai groups.
One possible confounding variable may be present in the selection of communities that were either selected by the program implementers (comparison area) or self-selected (intervention area was in the community where the request originated for an HIV prevention intervention). Either of these two methods of selection may indicate greater interest or awareness of HIV among the intervention communities and, thus, potentially a greater willingness to change HIV-related behaviors prior to the intervention.
Lastly, the highly sensitive nature of the study questions may have inhibited some of the respondents from answering survey questions, thereby limiting or skewing the data and analysis. Although some evidence of behavioral changes can be observed, many reported HIV-related sexual and traditional behavior changes are impossible to validate and, therefore, may not be a true representation of actual behaviors.
Our findings are limited to the study area, and are not directly generalizable to other Maasai or indigenous groups, however the results of the survey denote a highly effective contextualized intervention. It is promising for replication among other Maasai communities and for adaptation with indigenous people groups in other regions.
References
- Coast E. Wasting semen: Context and condom use among the Maasai. Cult Health Sex. 2007;9(4);387-401. Available from: http://dx/doi.org/10.1080/13691050701208474
- Mbugua T. The Maasai: Preserving culture and protecting girls. Global AIDSLink. 2007 Jan/Feb; 101:12-3.
- Coast E. Maasai demography [Ph.D. thesis]. University of London; 2001.
- Coast E. (Ereto-NPP). HIV/AIDS in Ngorongoro District. Report. [internet] ITAD, Lion House, Ditchling Common Industrial Estate Hassocks (England); 2002 Oct 7. Available from: http://www.ereto-npp.org/download_documents/
- May A, Ole Ikayo F. Wearing Illkarash: Narratives of image, identity and change among Maasai labour migrants in Tanzania. Dev Change. 2007; 275-98.
- Coast E. Local understandings of, and responses to, HIV: Rural-urban migrants in Tanzania. [Internet] Soc Sci Med. 2007; 63(4):1000-10. Available from: http://eprints.lse.ac.uk/archive/0000817
- Tanzania Commission for AIDS (TACAIDS). Tanzania HIV/AIDS and Malaria indicator survey. Dar es Salaam, Tanzania: National Bureau of Statistics (NBS). 2008.
- United Nations. Permanent forum on indigenous issues (fifth session), special theme: The millennium development goals, and indigenous peoples—redefining the goals
- Peter CM. Human rights of indigenous minorities in Tanzania and the courts of law. Int J Minor Group Rights. 2007; 14:455-87. http://dx.doi.org/10.1163/138548707X247428
- Kulzer JL. Socio-Cultural norms and acceptability of HIV/AIDS prevention strategies in the Simanjiro District of Tanzania. J Public and Int Affairs-Princeton. 2002; 13:82-103. Available from: http://www.princeton.edu/jpia/past-issues-1/2002/5.pdf
- May A. Maasai migrations: Implications for HIV/AIDS and social change in Tanzania. Boulder (CO): Institute of Behavioral Science; 2003, Jan 23. Available from: http://www.colorado.edu/ibs/pubs/pac/pac2003-0001.pdf
- United Nations. Indicators for monitoring the millennium development goals: Definitions, rationale, concepts, and sources. New York (NY): United Nations Publication; 2003. Available from: http://mdgs.un.org/UNSD/MDG/Resources/Attach/Indicators/HandbookEnglish.pdf
- The United Republic of Tanzania’s Prime Minister’s Office. National multisectoral HIV prevention strategy 2009-2012: ‘Towards achieving Tanzania without HIV’. November 2009. Available from: http://aidstar-one.com/sites/default/files/prevention/resources/national_strategic_plans/Tanzania_2009-2012_Prevention_Strategy.pdf
- Maddux J. Self-Efficacy: The power of believing you can. In: Snyder CR, Lopez SJ, editors. Handbook of positive psychology. New York (NY): Oxford University Press; 2002. p. 277-87.
- Depoy E, Gitlin LN. Introduction to Research. In: Understanding and Applying Multiple Strategies, 3rd ed. St Louis, MO: Elsevier Mosby; 2005. p. 241-52.