ORIGINAL ARTICLE
A preliminary investigation of the barriers to clean water access in the urban slums of Kolkata, India
Holly Anne Beistlinea
Abstract
Introduction: Safe drinking water is scarce in Kolkata. Inadequate knowledge and poor practices of storing and cleaning drinking water can cause severe effects on the health of the population. There is a need to understand the current trend of attitudes and practices of individuals living in urban slums to reduce water-borne diseases and mortality. This limited convenience sample study attempted to explore and identify areas for further study regarding the barriers of clean water access in urban slums of Kolkata, India.
Methods: This pilot cross-sectional study was conducted in Kolkata, India during July 2014. Five urban slums were selected based on proximity and cooperation from the community. A sample of 50 women was taken, representing the five slums, with a sample of 10 women taken from each slum.
Results: The majority (80%) of the participants said they regularly have enough water available to meet the needs of their household. Fifty-two percent of subjects received their water for drinking from a tap, hand pump, or time pump. Thirty percent had water pumped into their homes, and 18% purchased their water from a water truck. Fourteen percent said they did not treat their water because it was too time consuming, 40% said it was too much work, and 34% said it was not needed. Ninety percent said they felt it was important to clean their water, almost half (48%) thought their water was not clean, but only 42% used some method to clean their water. Many subjects (68%) stated they knew how to clean their water, but 66% were unaware that visible dirt is not an indicator of illness-causing bacteria in water.
Conclusions: More focus should be directed towards improving awareness and knowledge and changing attitudes, motivation, and perceived susceptibility to disease from water within slum communities in Kolkata, India.
Introduction
Access to improved drinking water is a main public health concern around the globe. The urban slums of Kolkata, India, present many unique public health challenges, among them the scarcity of safe drinking water. Less than half the house-holds within Kolkata have improved sanitation facilities.1 The United Nations rates India 120th for water quality among the 122 selected nations covered.2 UNICEF and World Health Organization report that 67% of Indian households do not treat their drinking water, even though it could be chemically or bacterially contaminated. This is concerning because only a quarter of the total population in India has drinking water on their premises.3
Diarrhea is the second leading cause of death globally in children under five years.4 In India, pneumonia and diarrhea account for 50% of deaths of children under five.5 It has been estimated that 15–20% of community diarrheal disease in developing countries is attributed to unsafe drinking water, with recent studies indicating even higher percentages of waterborne diarrheal disease.6 According to India’s National Family Health Survey from 2005-2006, the under-five mortality rate among the urban poor was 72 per 1000 live births, significantly higher than the overall urban average of 52 per 1000 live births.7 The major etiological agents accounting for over a million diarrheal deaths per year, particularly in developing countries, are Escherichia coli, Rotavirus, Vibrio cholerae, and species of Shigella, which are spread through contaminated water and food or from person to person.8
India is a lower middle income country, with a total population of 1.252 billion as of 2013.9 Kolkata is the capitol of West Bengal, a state of India. It is located on the eastern bank of Ganga River. Kolkata is the 7th biggest city of India in area and population.10 In the year 2000, approximately 21% of the total urban population of India lived in slums. Specifically in Kolkata, 86% of the poor live in slums.1 The government of India defined slums as “those areas where buildings are in any respect unfit for human habitation,” according to the Slum Act of 1956.11 Generally, slums consist of clusters of homes constructed with temporary building materials. Living conditions are difficult within the slums due to a lack of basic amenities such as many families sharing a common latrine, no official arrangements for water supply, and poor drainage systems.1,12 Registered or legal slums, “bustees,” are recognized by the Calcutta Metropolitan Corporation (CMC) because of the title of the land. Illegal or unauthorized slums are known as squatter settlements. Squatter settlements can be found along the sides of canals, garbage dumps, railway tracks, and roads.12
A study from 2012 tested water from various slum locations in Kolkata. Samples were taken from 117 main sources from taps and tube wells, 200 from stored water for drinking, and 200 from stored water for washing. When analyzed, 28% (56/200) stored drinking water samples and 8% (10/117) main water sources were found to be contaminated with fecal coliforms.6 They also stated that the tube wells were usually not very deep and did not penetrate the impervious layer of soil. Moreover, they concluded that low levels of personal and domestic hygiene led to extensive environmental contamination, resulting in contamination of these water sources.6,13 The southern portion of Kolkata is serviced by a 120MGD water treatment plant called Garden Reach Water Works (GRWW). The treated water from the plant is transported through dedicated lines to a number of booster pumping stations that in turn serves the consumer’s water networks. In total, 2.3 million residents are served through the present system.14
Until access to piped treated water is attained, water purification at the point of consumption or point-of-use water treatment, has emerged as a cost-effective approach to protect populations lacking safe water.15 Inadequate knowledge and poor practices of storing and cleaning drinking water can cause severe effects on the health of the population. For reduction of water-borne diseases and mortality, there is a need to understand the current trend of attitudes and practices of individuals living in urban slums.16 Many attempts have been made by the Indian government and non-governmental organizations (NGO’s) to change behaviors associated with water consumption, but there is still a lack of practice within the slums of Kolkata. In order to reduce child mortality in Kolkata associated with clean water, the behaviors and barriers of clean water access in urban slums must first be understood.
Methods
This pilot cross-sectional study was conducted in Kolkata, India, during July 2014. Five urban slums were selected conveniently based on proximity and cooperation from the community. A convenience sample of 50 women was taken from 5 different slums, with a sample of 10 women taken from each slum. Mothers were surveyed because they were the primary water gatherers.16 Women were contacted by selecting residences at random throughout each slum community. Mothers that gave oral informed consent after the study’s purpose was explained to them were included in the study. If no eligible participant was found at the time of interview, an additional household was chosen. All interviews were conducted during the late afternoon when the mothers were more likely to be home. Confidentiality of the participants was maintained by assigning a number to each of the participants.
Preliminary data were gathered concerning basic household information such as the type of slum, age, religion, how many children under the age of 5 the participants had, and how many individuals lived in their household. Next, information was gathered about individuals’ attitudes towards water treatment practices. The variables contained in the survey included topics related to water safety, effects of unsafe drinking water on health, and the practices that were adopted to make water safe to drink. A participatory appraisal was used to collect information about the type of slum, estimated total population, average family size, educational systems available, average household income, surrounding environment, the various sources of drinking water, distance of water source from household, timings of water supply, and water storage practices. Slum number 1, Udayan Polly, received drinking water from daily deliveries via a water truck. Each tank held 3,600 liters of water and required each community to deposit $7.50 (about 450 rupees) per tank.10 Water samples taken from water pumps within slum number 1 found high fecal contamination, 100-1000 E. coli per liter of water. Water was tested at Water Testing Lab Deo Tech in Kolkata. Water samples were collected from slum number 5, Mudapara, by Kolkata City Mission on July 10, 2014. This sample was tested at N.D. International in Kolkata. No high levels of E. coli or other harmful coliforms were detected in the sample taken from a timed water tap within the slum number 5 community.
The Health Belief Model (HBM) is based on the concepts that health-related interventions will only be effective if recipients are aware of their susceptibility to disease and feel they are capable of taking a role in addressing the problem.17 Using the Health Belief Model, a questionnaire was con-structed based on the perceived seriousness, perceived susceptibility/perceived threat, perceived benefits, perceived barriers, cue to action, and self-efficacy associated with clean water. The survey comprised of the following sections:
- Household data: Age of the subject, household size, and the number of infants living in the household.
- Water practices: Information was gathered about the main source of water, quantity and quality available, if any methods are used to clean water, and reasons why they do not treat their water.
- Water knowledge: Attitudes and beliefs of drinking water’s cleanliness, knowledge of how to clean water, how to tell if the water is clean, knowledge of consequences of drinking contaminated water, and number of known cases of stomach illness within the last year.
Data collected from the questionnaire were analyzed in order to understand the behaviors and barriers associated with clean water in Kolkata slums. Descriptive analysis was performed using IBM SPSS Statistics Program version 22. Chi-square analysis was performed to compare the qualitative variables using IBM SPSS Statistics Program version 22.
Results
A total of 50 participants were enrolled in the study conducted in July 2014 in urban poor slum settings in Kolkata, India. The mean age of the participants was 30.46 years (SD=11.56), with a mean family size of 5 individuals (SD=0.64), and a mean of 1.49 children below the age of 5 years per household (SD=0.54) (Table 1).
Table 1. Household descriptive data Kolkata, India slums, 2014
Min |
Max |
Mean |
Standard Deviation |
|
Respondent Age (years) |
17 |
75 |
30.46 |
11.56 |
Family Size |
1 |
8+ |
5.00 |
0.64 |
Number of Infants |
0 |
5 |
1.49 |
0.54 |
Note: N=50
The majority (80%) of the participants said they regularly had enough water available to meet the needs of their household. Results showed that 52% of the subjects received their water for drinking from a tap, hand pump, or time pump. Thirty percent had water pumped into their homes, and 18% purchased their water from a water truck. Additionally, only 4% used water filters to purify their drinking water, while 36% boiled, 2% used chlorine or iodine, and a little over half (58%) of the subjects did not treat their water at all (Figure 1). Fourteen percent said they did not treat their water because it was too time consuming, 40% said it was too much work, and 34% said it was not needed (Table 2).
Figure 1. Method used to treat water in slum homes Kolkata, India prior to consumption, 2014
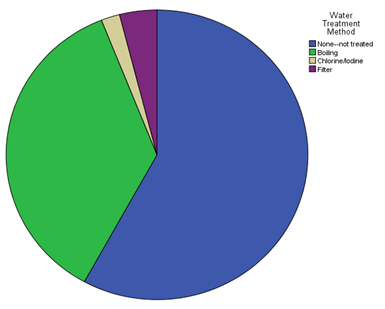
Table 2. Water practices in slum homes Kolkata, India, 2014
| Variables | Results |
|---|---|
| 1. Do you have enough water regularly available to meet the needs of your household? | |
| a. Always | 80% (n=40) |
| b. Most of the time | 6% (n=3) |
| c. Sometimes | 14% (n=7) |
| 2. What is the main source of water for drinking and cooking in your household? | |
| a. Pump/tap/well | 52% (n=26) |
| b. Piped into home | 30% (n=15) |
| c. Water Truck | 18% (n=9) |
| 3. What method, if any, is used to treat the water prior to human consumption? | |
| a. None - not treated | 58% (n=29) |
| b. Boiling | 36% (n=18) |
| c. Chlorine/Iodine | 2% (n=1) |
| d. Filter | 4% (n=2) |
| 4. If you do not treat your water before drinking, why? | |
| a. Time consuming | 14% (n=7) |
| b. Too much work | 40% (n=20) |
| c. Not needed | 34% (n=17) |
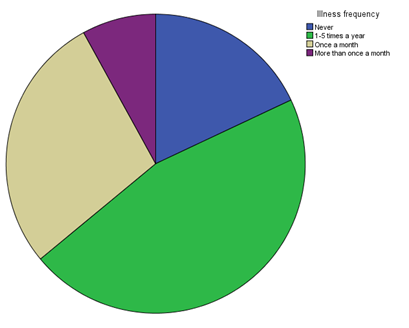
A little more than half (55%) of the subjects reported themselves or their children experienced stomach illness and diarrhea 1-5 times a year, 22.5% said once a month, 10% reported more than once a month, and 12.5% reported never (Figure 2).
Figure 2. Reported stomach illness & diarrhea frequency for respondents and children in slum Kolkata, India, 2014
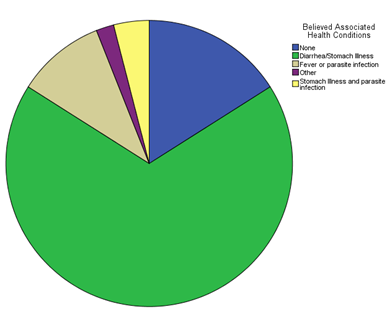
The subjects’ water knowledge is outlined in Table 3. Most (88%) participants said that some sort of stomach illness was associated with their water source (Figure 3). The majority, (90%) felt it was important to clean their water before drinking (Table 3).
Table 3. Clean drinking water knowledge and beliefs in slum homes Kolkata, India, 2014
| Variables | Results |
|---|---|
| 1. What health conditions are generally thought to be associated with the use of water from this source? | |
| a. None | 16% (n=8) |
| b. Stomach illness/diarrhea | 68% (n=34) |
| c. Fever or parasite infection | 10% (n=5) |
| d. Both diarrhea/stomach illness and fever/parasite infection | 4% (n=2) |
| 2. How many times a year do you or your children experience stomach illness and diarrhea? | |
| a. Never | 18% (n=9) |
| b. 1-5 times/year | 46% (n=23) |
| c. Once a month | 28% (n=14) |
| d. More than once a month | 8% (n=4) |
| 3. Do you think your drinking water is safe? | |
| a. Yes | 48% (n=24) |
| b. No | 48% (n=24) |
| c. Don’t Know | 4% (n=2) |
| 4. Do you feel it is important to clean your water before drinking? | |
| a. Yes | 90% (n=45) |
| b. No | 10% (n=5) |
Figure 3. Heath conditions thought to be associated with respondent’s source of drinking water in slum Kolkata, India, 2014
In answering the question on whether or not you can tell if your water is contaminated, 66% thought it was possible to tell if drinking water is dirty simply by looking and seeing visible dirt, while 34% understood that it was not possible to tell if drinking water was dirty just by looking at it. Sixtyeight percent said they knew how to clean their water, and 24% said they did not know how to clean their water (Table 4).
Table 4. Clean drinking water knowledge and beliefs in slum homes Kolkata, India, 2014 continued
| Variables | Results |
|---|---|
| 1. How can you tell if your water is contaminated? | |
| a. Visible dirt | 66% (n=33) |
| b. Can’t tell just by looking | 34% (n=17) |
| 2. Do you know how to clean your water? | |
| a. Yes | 68% (n=34) |
| b. No | 24% (n=12) |
There was a significant relationship between each slum and the belief that their water was safe. The majority in slums 1 and 2 felt their water was safe, while majority in slums 3, 4, and 5 felt their water was not safe (Table 5). There was a significant relationship between water source of tap/well/pump and the belief that it was not safe (Table 6).
Table 5. Belief of safe water vs. slum chi-square contingency table
| Slum | Total | |||||||
|---|---|---|---|---|---|---|---|---|
| 1.00 | 2.00 | 3.00 | 4.00 | 5.00 | ||||
| Safe | Yes | 7 | 9 | 2 | 3 | 3 | 24 | |
| 29.2% | 37.5% | 8.3% | 12.5% | 12.5% | 100.0% | |||
| No | 1 | 1 | 8 | 7 | 7 | 24 | ||
| 4.2% | 4.2% | 33.3% | 29.2% | 29.2% | 100.0% | |||
| Don’t know | 2 | 0 | 0 | 0 | 0 | 2 | ||
| 100.0% | 0.0% | 0.0% | 0.0% | 0.0% | 100.0% | |||
| Total | 10 | 10 | 10 | 10 | 10 | 50 | ||
| 20.0% | 20.0% | 20.0% | 20.0% | 20.0% | 100.0% | |||
| p=.001 | ||||||||
Table 6. Water source vs. belief if safe to drink chi-square contingency table
| Safe | Total | |||||
|---|---|---|---|---|---|---|
| Yes | No | Don't know | ||||
| Source | Pump/tap/well | 11 | 15 | 0 | 26 | |
| 42.3% | 57.7% | 0.0% | 100.0% | |||
| Piped into home | 6 | 8 | 0 | 14 | ||
| 42.9% | 57.1% | 0.0% | 100.0% | |||
| Water truck | 6 | 1 | 2 | 9 | ||
| 66.7% | 11.1% | 22.2% | 100.0% | |||
| Other | 1 | 0 | 0 | 1 | ||
| 100.0% | 0.0% | 0.0% | 100.0% | |||
| Total | 24 | 24 | 2 | 50 | ||
| 48.0% | 48.0% | 4.0% | 100.0% | |||
| p=.026 | ||||||
Discussion
Water is essential for life. We all have know-ledge and instinct of its necessity for drinking, producing food, washing, and maintaining our health.2 The 2011 Census of India reveals that 17.4% of urban households in India live in slums. The increasing number of slum-dwellers poses serious challenges to the provision of basic urban water services.18 The water supply in Kolkata and most other Indian cities is only available for a few hours per day, pressure is irregular, and the quality of water is questionable.19 With understanding of the attitudes, beliefs, and knowledge of drinking water in slums, communities can be mobilized to work towards improved drinking water facilities, as well as being taught about drinking water contamination risks at the household level and safe storage of drinking water from unreliable supplies.2
This pilot study attempted to assess the present situation of clean water and associated knowledge, attitudes, and beliefs within the slums of Kolkata, India. Based on the results obtained from the questionnaire, there is a lack of motivation associated with clean water in the slum communities of Kolkata. Ninety percent said they felt it was important to clean their water, almost half (48%) believed their water was not clean, but only 42% used some method to clean their water. Many subjects (68%) stated they knew how to clean their water, but 66% were unaware that visible dirt was not an indicator of illness-causing bacteria in water. Respondents identified present barriers to clean water as too time consuming (14%) and too much work (40%). Based on the questionnaire, information and knowledge about clean water was not lacking for many participants. However, this raises a more difficult challenge of addressing the motivation and will to clean water. Perceived susceptibility of disease from contaminated water needs to be addressed as well. There is knowledge of poor water sources and the illness they cause, but perceived susceptibility to disease is not sufficient enough to motivate people to action.
There were several limitations of the current study such as small sample size, language barrier, and the use of interpreters. Any time a convenience sample is used, it may confound the analysis because subjects were chosen based on availability rather than being representative of the full population. Further research should be done on water storage practices and the knowledge associated with water handling, hygiene, and storage contamination. If water is not piped directly into a house whenever needed, it must be stored in containers. This provides a number of opportunities for contamination.20 Problems associated with inadequate water supplies are further complicated by poor sanitation, which can cause water to become contaminated. In urban areas, many slums contain limited, crowded public latrines that are distant from many of the dwellings they serve, causing many people to defecate in the open.18 Additional data should be collected on the practices and attitudes and beliefs associated with sanitation within slum communities as well as different methods of cleaning water. For example, in one conversation with a subject, she stated that she thought her roof was too dirty to effectively execute the Solar Water Disinfection (SODIS) method, which is a process that uses solar radiation to heat and disinfect water stored in plastic bottles.15
Eventually, the provision of safe, sustainable, drinking water needs to be achieved within the slum communities of Kolkata. Movement needs to be made from point-of-use water treatment to more sustainable means. Communities need to be mobilized towards creating their own means of sustainable water. A study was performed in Kolkata in 2007 that investigated the current water situation and respondents’ willingness to pay for sustainable water. Half of the 202 people surveyed in this study were slum dwellers while the other half were apartment dwellers. A weighted average of the willingness to pay for drinkable water was analyzed and compared to the cost of providing potable water. The willingness to pay exceeded the production and maintenance cost for the drinkable water supply scheme suggesting that a water tariff is economically justifiable.21 This study shows that communities in Kolkata are willing to pay and work toward sustainable clean water, but more knowledge and awareness needs to be raised to mobilize communities towards action.
Conclusion
Water management solutions exist that can make significant strides in combating both disease and mortality. Recommendations based on infor-mation gained from this study include creating more awareness of the level of contamination of water in the slums, creating community groups for women to learn about using point-of-use water treatment methods, decreasing pathways of contamination, and mobilizing communities to work towards sustainable clean water systems.
Further research should be done on water storage practices and the knowledge associated with water handling, hygiene, and storage contamination, as well the practices, attitudes, and beliefs associated with sanitation within slum communities. Further research should also be performed regarding the motivation and will to clean water within the slums. In order to reduce child mortality in Kolkata, India associated with clean water, the behaviors and barriers of clean water access in urban slums must first be understood. More focus should be directed towards improving the awareness, knowledge, and changing attitudes of motivation and perceived susceptibility to disease from water within slum communities in Kolkata, India.
References
- Goli S, Arokiasamy P, Chattopadhayay A. Living and health conditions of selected cities in India: setting priorities for the National Urban Health Mission. Cities [Internet]. June 2011 [cited 2014 July 18];28:461-9. Available from: http://www.sciencedirect.com.ezproxy.liberty.edu:2048/science/article/pii/S0264275111000631. http://dx.doi.org10.1016/j.cities.2011.05.006
- United Nations. Water for people water for life: the United Nations world water development report. World Water Assessment Programme. 2003 [cited 2014 July 18]. Available from: http://unesdoc.unesco.org/images/0012/001297/129726e.pdf.
- WHO/UNICEF. Joint Monitoring Programme (JMP) update for 2014. Progress on drinking water and sanitation. May 2014 [cited 2014 August 20]. Available from: http://www.who.int/water_sanitation_health/publications/2014/jmp-report/en/.
- Manna B, Nasrin D, Kanungo S, et al. Determinants of health care seeking for diarrheal illness in young children in urban slums of Kolkata, India. Am. J. Trop. Med. Hyg. [Internet]. July 2013 [cited 2014 July 18];89(1):56-61. Available from: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3748502/?tool=pmcentrez&report=abstract. http://dx.doi.org/10.4269/ajtmh.12-0756.
- Chatterjee A, Paily VP. Achieving Millennium Development Goals 4 and 5 in India. BJOG [Internet]. 2011 [cited 2014 July 17];118(2):47–59. Available from: http://onlinelibrary.wiley.com.ezproxy.liberty.edu:2048/doi/10.1111/j.1471-0528.2011.03112.x/full. http://dx.doi.org/10.1111/j.1471-0528.2011.03112.x.
- Palit A, Batabyal P, Kanungo S, Sur D. In-house contamination of potable water in urban slum of Kolkata, India: a possible transmission route of diarrhea. Water and Science Technology [Internet]. February 2012 [cited 2014 July 18]:66(2);299-303. Cited in PubMed; PMID 22699333. http://dx.doi.org/10.2166/wst.2012.177.
- Gupta K, Arnold F, Lhungdim H. Health and living conditions in eight Indian cities. National Family Health Survey (NFHS-3) India 2005-06. Ministry of Health and Family Welfare Government of India. August 2009 [cited 2014 July 17]. http://www.nfhsindia.org.
- Qadri F, Svennerholm AM, Faruque ASG, Sack RB. Enterotoxigenic Escherichia coli in developing countries: epidemiology, microbiology, clinical features, treatment, and prevention. Clinical Microbiology Reviews [Internet]. July 2005 [cited 2014 July 17]:18(3);465-83. Available from: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1195967/?tool=pmcentrez&report=abstract. http://dx.doi.org/10.1128/CMR.18.3.465–483.2005
- The World Bank. Data: India. 2013 [cited 2014 August 18]. http://data.worldbank.org/country/india.
- Kolkata Municipal Corporation. https://www.kmcgov.in/KMCPortal/jsp/KMCPortalHome1.jsp. [cited 2014 August 20].
- Parliament of the Republic of India. The slum areas (improvement and clearance) Act. 1956 (Act No. 96 of 1956) [cited 2014 August 18]. http://lawmin.nic.in/legislative/textofcentralacts/1956II.pdf.
- Kundu, N. The case of Kolkata, India. Understanding slums: case studies for the Global Report on Human Settlements. UN-Habitat. Earthscan, London. 2003 [cited 2014 August 20];195-228. http://www.ucl.ac.uk/dpu-projects/Global_Report/cities/kolkata.htm.
- Sur D, Sarkar BL, Manna B, et al. Epidemiological, microbiological & electron microscopic study of a cholera outbreak in a Kolkata slum community. Indian J Med Res [Internet]. January 2006 [cited 2014 July 18]:123;31-6. Available from: http://www.ncbi.nlm.nih.gov/pubmed/16567865.
- Roy KD, Thankur B, Konar TS, Chakrabarty SN. Rapid evaluation of water supply project feasibility in Kolkata, India. Drink. Water Eng. Sci [Internet]. March 2010 [cited 2014 July 18]:3;29–42. Available from: http://www.drink-water-eng-sci.net/3/29/2010/dwes-3-29-2010.pdf. http://dx.doi.org/10.5194/dwes-3-29-2010.
- Fiebelkorn AP, Person B, Quick RE, et al. Systematic review of behavior change research on point-of-use water treatment interventions in countries categorized as low- to medium-development on the human development index. Soc Sci Med [Internet]. August 2012 [cited 2014 July 17]:75(4);622-33. Available from: http://www.sciencedirect.com.ezproxy.liberty.edu:2048/science/article/pii/S0277953612001815. http://dx.doi.org/10.1016/j.socscimed.2012.02.011.
- Joshi A, Prasad S, Kasav JB, Segan M, Singh AK. Water and sanitation hygiene knowledge attitude practice in urban slum settings. Global J Health Sci [Internet]. November 2013 [cited 2014 July 17];6(2):23-34. Available from: http://www.ncbi.nlm.nih.gov/pubmed/24576362. http://dx.doi.org/10.5539/gjhs.v6n2p23.
- Martin JH, Elmore AC. Water drinking attitudes and behaviors in Guatemala: an assessment and intervention. J Rural Trop Pub Heal [Internet]. 2007 [cited 2014 June 27];6:54-60. http://www.jcu.edu.au/jrtph/vol/v06martin.pdf.
- Satapathy BK. Safe drinking water in slums: from water coverage to water quality. Economic & Political Weekly [Internet]. June 2014 [cited 2014 August 9]:69(24);50-5. http://www.academia.edu/7288971/Safe_Drinking_Water_in_Slums_From_Water_Coverage_to_Water_Quality.
- McKenzie D, Raya I. Urban water supply in India: status, reform options and possible lessons. Water Policy [Internet]. July 2009 [cited 2014 July 18];11(4):442-60. Available from: http://www.iwaponline.com/wp/01104/wp011040442.htm. http://dx.xoi.org/10.2I66/wp.2009.056.
- Bartlett S. Water, sanitation and urban children: the need to go beyond “improved” provision. Environment & Urbanization [Internet]. October 2003 [cited 2014 August 9];15(2):57-70. Available from: http://eau.sagepub.com/content/15/2/57.full.pdf. http://dx.doi.org/10.1177/095624780301500220.
- Guha S. Valuation of clean water supply by willingness to pay method in a developing nation: a case study in Calcutta, India. Journal of Young Investigators [Internet]. October 2007 [cited 2014 August 23]. http://www.jyi.org/issue/valuation-of-clean-water-supply-by-willingness-to-pay-method-in-a-developing-nation-a-case-study-in-calcutta-india/
www.cjgh.org